Physical Address
304 North Cardinal St.
Dorchester Center, MA 02124
Physical Address
304 North Cardinal St.
Dorchester Center, MA 02124

If you’ve been told you need a tooth replaced, you’ve probably come across the term “dental implant” — but the type most people receive, and the type most dentists are referring to, is specifically an endosteal implant. Understanding what that means, how the procedure works, and who it suits can help you have a more informed conversation with your periodontist or oral surgeon.
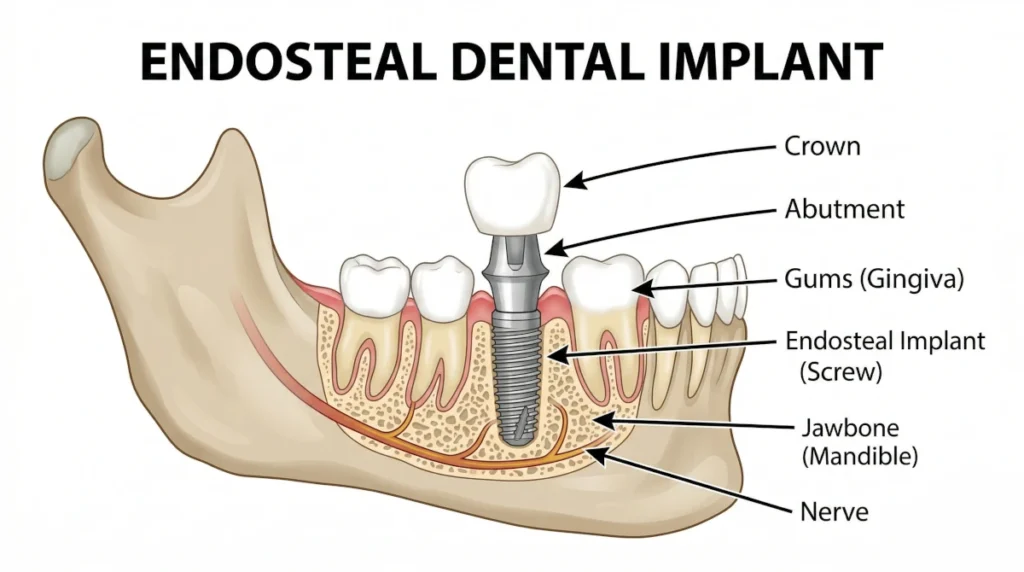
The word endosteal comes from the Greek roots for “within” and “bone.” An endosteal implant is a small titanium post that is surgically placed directly into the jawbone, where it acts as an artificial tooth root.
Once the implant is in place, the surrounding bone gradually fuses to it through a process called osseointegration. This bond is what gives the implant its stability — it becomes a fixed part of your jaw rather than sitting on top of it or relying on adjacent teeth for support.
After osseointegration is complete (typically over several months), a connector piece called an abutment is attached to the post. A custom-made crown is then fitted over the abutment, completing the restoration. The end result looks, feels, and functions like a natural tooth.
Endosteal implants are the most widely used implant type. The alternative — subperiosteal implants, which sit on top of the jawbone under the gum — is rarely used today and is generally reserved for patients who cannot undergo bone grafting.
Endosteal implants can replace a single missing tooth, multiple teeth, or serve as anchors for implant-supported bridges and dentures. They’re used to address tooth loss from:
Unlike removable dentures, implants don’t shift or require adhesives. Unlike bridges, they don’t require grinding down healthy adjacent teeth. For most patients, they’re considered the gold standard for tooth replacement.
Treatment typically unfolds over several months, though timelines vary depending on your individual case and whether any preparatory work — such as bone grafting or tooth extraction — is needed first.
Initial assessment: Your provider will take X-rays or a cone beam CT scan to evaluate your jawbone density and volume, gum health, and overall oral anatomy. This determines whether you’re a suitable candidate and helps plan the implant position precisely.
Surgical placement: The implant post is inserted into the jawbone under local anaesthesia. Most patients report the procedure itself is more comfortable than anticipated — post-operative soreness for a few days is typical.
Osseointegration: This is the waiting period, usually three to six months, during which the bone fuses to the implant. During this time, a temporary crown or prosthetic may be placed to maintain aesthetics and function.
Abutment and crown placement: Once osseointegration is confirmed, the abutment is attached and impressions are taken for your permanent crown. The final restoration is fitted and adjusted for bite and comfort.
Endosteal implants are suitable for a wide range of patients, but a few key factors determine candidacy.
Sufficient bone volume Because the implant anchors into the jawbone, there needs to be enough bone present to support it. Bone loss is common after tooth extraction — the jaw begins to resorb without a tooth root to stimulate it. If significant resorption has occurred, bone grafting may be recommended before implant placement. This adds time to the process but doesn’t necessarily rule out implants.
Healthy gums Active gum disease is a contraindication for implants. Periodontitis creates a bacterial environment that can interfere with osseointegration and increase the risk of peri-implantitis — an inflammatory condition around the implant similar to gum disease. If periodontal disease is present, it needs to be treated and stabilised before implant surgery is considered.
General health Certain systemic conditions and medications can affect healing. Uncontrolled diabetes, bisphosphonate use (commonly prescribed for osteoporosis), and autoimmune conditions affecting bone metabolism are all factors your provider will weigh. Heavy smoking significantly impairs healing and increases implant failure rates — most providers will discuss this candidly if it applies to you.
Completed jaw growth Implants aren’t recommended for patients whose jawbones are still developing. This typically means treatment is deferred until the late teens or early adulthood.
If you don’t immediately qualify, that doesn’t automatically mean implants are off the table. In many cases, preparatory treatments — bone grafting, gum disease therapy, or medical management — can bring you to a point where implants become viable.
Endosteal implants have a strong track record. Studies consistently report survival rates above 95% at ten years when placed in appropriate candidates and maintained well. Regular dental check-ups, proper home care, and not smoking all contribute significantly to long-term outcomes.
Implants can last decades — in many cases, a lifetime — making them a cost-effective option when considered over time despite the higher upfront investment compared to bridges or dentures.
If you’re considering an endosteal implant, a consultation with a periodontist or oral surgeon is the right starting point. They’ll assess your bone health, gum status, and medical history to determine whether implants are appropriate — and if not immediately, what steps could get you there.
The right candidate, properly treated, can expect a restoration that is indistinguishable from a natural tooth and built to last.