Physical Address
304 North Cardinal St.
Dorchester Center, MA 02124
Physical Address
304 North Cardinal St.
Dorchester Center, MA 02124

If you’re researching full-arch tooth replacement, you’ve probably come across both All-on-4 and 3-on-6. They get mentioned together, sometimes as near-equivalents, but they are actually different treatments built around different assumptions about your bone, your anatomy, and what your jaw looks like right now.
Below is a breakdown of how each system works, who qualifies, what the clinical evidence shows, and where the differences show up in daily life.
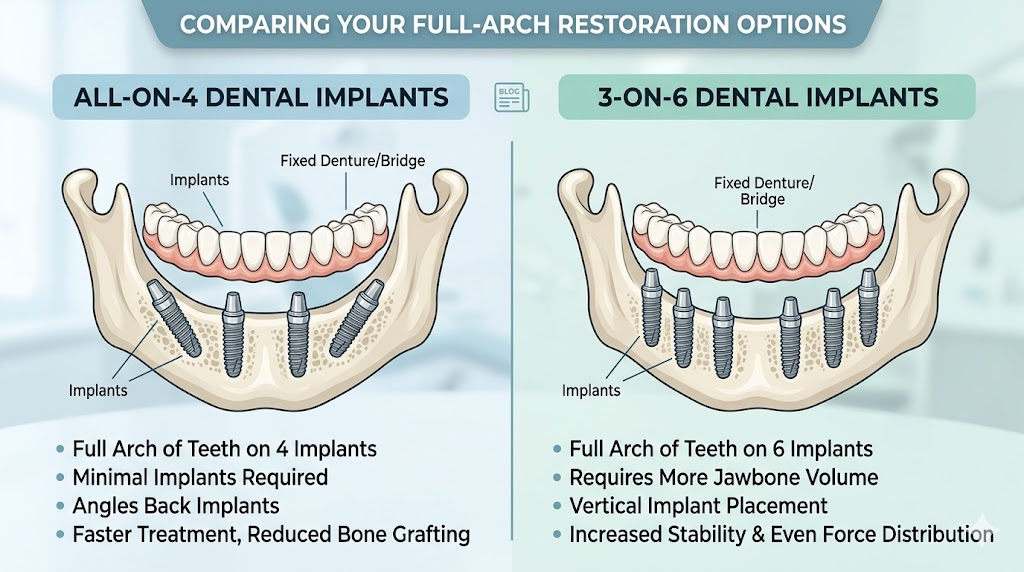
All-on-4 uses four implants per arch to support a single fixed prosthesis. Two implants sit vertically near the front of the jaw, and two are placed at an angle of around 30 to 45 degrees toward the back. The angled placement isn’t arbitrary — it allows those rear implants to reach denser bone further forward in the jaw, avoiding the posterior region where bone is often thinner and where the maxillary sinuses sit in the upper arch. The prosthesis covers the full arch and typically includes a pink acrylic base that replaces missing gum tissue.
3-on-6 uses six implants per arch to support three separate bridges rather than one continuous prosthesis. The arch is divided into three sections, each bridge sitting on two implants placed vertically. Because the bridges cover only the crown area without a gum-coloured base, the result can look more like natural teeth when the patient’s own gum tissue is still intact and healthy. Maintenance is also different: the separate bridges can be brushed and flossed much like natural teeth, without removal.
This is where the two treatments diverge most clearly, and where patient expectations sometimes run ahead of clinical reality.
All-on-4 was designed to work in patients who have experienced bone loss. The angled posterior implants sidestep areas of resorption that would otherwise make placement difficult or impossible. This means the treatment can be offered to a wider range of patients, including those who have worn dentures for years and have lost significant bone volume. Bone grafting is not required in most cases, which reduces both cost and recovery time.
3-on-6 requires substantially better bone conditions. Because six implants are placed vertically and spread across the arch, there needs to be sufficient bone height and density at each placement site. Patients who have experienced notable bone loss, worn complete dentures for an extended period, or have significant gum recession are often not candidates. One clinical description puts it directly: if you have had dentures for a while, you are likely missing bone and gum tissue, and 3-on-6 is not an option at all.
The patient population who can actually receive 3-on-6 is narrower than most marketing material suggests. It fits patients whose teeth need extraction but whose jaw bone is still in good condition — a combination that describes relatively few people presenting for full-arch replacement.
All-on-4 has an unusually deep body of clinical data behind it. Long-term follow-up studies spanning 10 to 18 years have been published, and the numbers are consistent. A 2011 study in the Journal of the American Dental Association reported implant survival rates of 94.8% at five years and 93.8% at 10 years in mandibular All-on-4 restorations. Subsequent data from the Malo Clinic group showed prosthesis survival rates of 98.8% at 10 years. Maxillary outcomes come in slightly lower but still high, with survival rates in the 94 to 97% range across 5 to 13 years of follow-up. Average marginal bone loss at 10 years has been documented at approximately 1.7mm, which falls within acceptable clinical parameters.
Those figures measure implant survival — whether the implant stays in place. The broader complication picture is a little less clean. Research published in Decisions in Dentistry found that biologic complication rates run between 18.9% and 25.5%, and mechanical complication rates between 7.3% and 36.7%. Prosthesis fractures, screw loosening, and soft tissue issues around implants are real possibilities over a decade or more of function. They’re manageable with regular monitoring, but patients should know going in that some degree of maintenance is part of the long-term picture.
3-on-6 has considerably less published data. There are no equivalent long-term follow-up studies from independent groups comparable to what exists for All-on-4. The clinical case for 3-on-6 rests more on biomechanical reasoning — six implants distributing force across a wider area — and shorter-term outcomes than on decade-long evidence.
A finite element analysis study comparing All-on-4 and All-on-6 configurations did find lower stress values with six implants versus four, which supports the biomechanical logic behind adding more implants. But stress modelling is not the same as long-term clinical follow-up, and six implants placed in patients with good bone is a different clinical scenario from four angled implants in patients with moderate bone loss.
For patients with good bone and healthy gum tissue, 3-on-6 has a genuine aesthetic edge. Because the bridges cover only the teeth without an artificial gum base, the result can look more natural — there’s no pink acrylic collar sitting above the teeth. For patients who still have good gum contours, this makes a visible difference and matters a lot to some people.
All-on-4 includes that gum-coloured base as part of the prosthesis design, partly to replace missing soft tissue and partly because the single-arch prosthesis needs it for support and appearance. For patients with significant bone and tissue loss, this is actually an advantage: it fills the space that would otherwise leave an unnatural gap between the prosthesis and the face. For patients with better bone who might have qualified for 3-on-6, some find the appearance less natural-looking than they’d hoped for.
Daily maintenance differs in a practical way. All-on-4 prostheses are fixed and not removed by the patient, but because the single arch sits close to the gum, cleaning underneath takes some effort. Water flossers and specialised cleaning tools are typically recommended. 3-on-6 bridges can be maintained with regular brushing and flossing at home, which most patients find more intuitive.
The tradeoff with 3-on-6 is that each bridge sits on only two implants. If one of those implants fails — particularly in the middle section — the entire bridge it supports becomes unstable. That’s a more disruptive failure mode than what you’d see in an All-on-4 design, where the single prosthesis can often still function while the problem is addressed.
3-on-6 generally costs more than All-on-4, because it involves more implants and a more technically demanding placement. All-on-4 was partly designed around reducing surgical complexity and total implant count, which keeps costs lower. For patients who qualify for both options, cost is often the deciding factor.
Good All-on-4 candidates are typically patients with moderate to severe bone loss, those who have worn full dentures, and those who want a fixed result as quickly as possible without bone grafting. The treatment covers a wide range of presentations and has decades of data supporting predictable outcomes.
Patients considered for 3-on-6 tend to have healthy bone architecture, have not experienced significant recession, and are coming in for extraction of failing teeth rather than replacement of long-standing tooth loss. The aesthetic upside is real for this group, and the maintenance routine suits patients who want something as close to natural teeth as possible.
What matters more than counting implants is the quality of the clinical workup. Both treatments require careful imaging, bone assessment, and surgical planning. For All-on-4, the angled placement depends on precise execution. For 3-on-6, the six implants need to be positioned consistently for the bridges to seat correctly — a different kind of precision, but no less demanding.
All-on-4 has the evidence advantage. Its long-term data, wide candidacy range, and well-documented outcomes make it easier to plan around for most patients. The complication rates over time are real and worth discussing with your provider, but they don’t change the overall picture.
3-on-6 offers a genuinely different experience for patients who qualify — better aesthetics in the right case, more familiar maintenance, and a segmented design some patients find more natural-feeling. The evidence base is thinner, and the qualifying criteria are stricter. It’s not a better version of All-on-4 for everyone; it’s a different treatment that suits a smaller group of patients.
If you’re weighing either option, the first question to resolve is not which system you prefer, but whether your bone and anatomy support the one you’re leaning toward. A CBCT scan and a consultation with an experienced implant provider is the only reliable way to find out.Share